3,396 Children: A Story Kenya Must No Longer Accept
Jun 20, 2026
story
Seeking
Collaboration

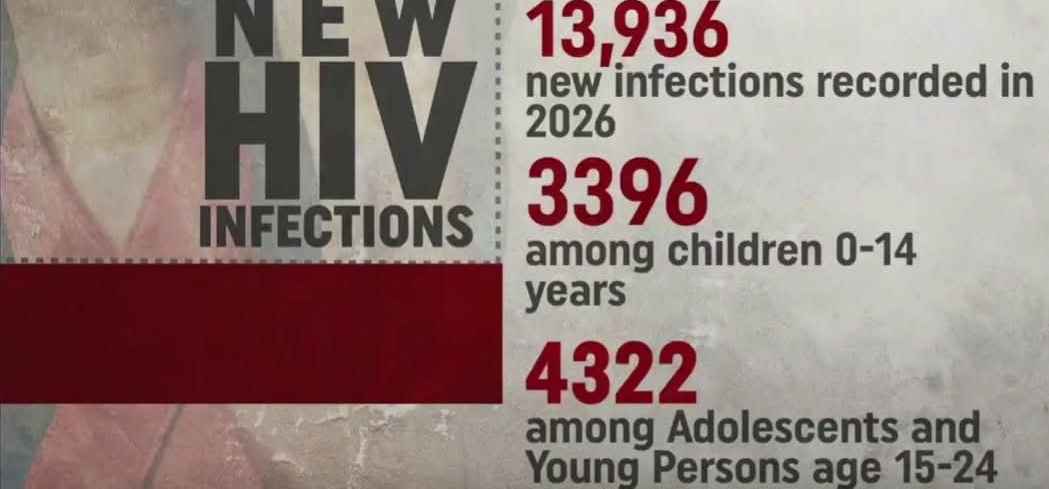
Photo Credit: Kristine Yakhama
I first sit with the number the way elders sit with silence before speaking of something that cannot be rushed. 3,396. It does not arrive as a statistic so much as a presence—heavy, unsettling, impossible to ignore. In Kenya in 2026, this is the number of children newly infected with HIV. Not a historical echo, not a distant projection, but today’s reality written into the lives of children who should have been entering the world free of it. In many homes, that number would feel less like data and more like a school register read aloud under a morning sun—names that should have become laughter, footsteps, and dreams, but instead become entries in a report no parent ever wanted to face. And so the mind asks a question older than policy itself: when a roof keeps leaking on the same family, do we continue blaming the rain, or do we finally admit the house was never properly repaired?
Before any statistic, there is always a journey. A mother wakes before the sun has fully risen, ties a shawl around her shoulders, lifts a child onto her back, and begins walking. The road stretches long—sometimes dusty, sometimes muddy, always uncertain—but she walks because hope is never still; it moves. There is a proverb: “A child belongs to the community.” Yet on this path, she often walks as if she belongs to no one but her determination. She is not walking for herself alone. She is walking for a child not yet born, or a child already growing within her, or a child she prays will never have to swallow the same pills she has learned to survive on. Each step feels like a negotiation between hope and fate, as though the future depends on whether she arrives in time.
And yet the data tells a harder truth. Nearly a quarter of new infections are children aged 0–14, and when adolescents and youth are included, more than half of all new infections in Kenya are among the young. It is as if the river of tomorrow is being quietly diverted before it ever reaches the sea. We know what prevents this. The science is not missing, and the tools are not unknown. What is missing is not knowledge but consistent delivery—systems that reach women early, stay with them, and do not break at the very point where continuity matters most. There is a Swahili saying: “Haraka haraka haina baraka.” But here, it is not haste that harms us; it is delay—delay in access, delay in treatment, delay in action.
I think of the mothers who walk long distances under a merciless sun, a child tied to their backs, another life growing inside them, and hope carried quietly like a fragile calabash. Some arrive in time, and some do not—not because they failed, but because the system did not arrive with them. There is another proverb: “Mwenda pole hajikwai.” Yet what happens when it is not the mother who is slow, but the system that moves too late to meet her urgency? Clinics should be places of reassurance, but too often they become spaces of waiting—queues, stockouts, referrals, and instructions to return another day, as though the virus itself respects schedules.
A more difficult truth sits beneath all of this: nearly 38% of mother-to-child transmissions occur simply because the mother was not on ART. Not refusal, not neglect, but absence—absence of access, absence of continuity, absence of a system that held her from pregnancy through breastfeeding without breaking the chain of care. And so we must ask how many of these infections were ever preventable, and how many were simply allowed to happen through delay. As elders say, “A small crack in the wall brings down the house,” and here the crack is no longer small.
I have sat in rooms where decisions are made carefully, where words are softened so they do not disturb comfort, and urgency is absorbed into procedure. I have spoken plainly that pregnant and breastfeeding women are not a side concern but the very centre of prevention, and I have watched those words become “noted.” Yet “noted” does not restock a clinic, does not reach a rural mother at dawn, does not prevent transmission in the moment it matters most. There is a proverb: “Words are like eggs; once broken, they cannot be gathered again.” But here, it is not only words that are breaking—it is trust, stretched thin between knowledge and action.
Kenya’s mother-to-child transmission rate stands at 8.04%, above the global target of below 5%. On paper, it appears like a narrow gap, but in reality, it is the distance between a child born free and a child born into lifelong treatment. A small crack, yes—but as the saying goes, even a small leak can sink a great ship. And so we find ourselves watching that leak widen, not because we do not know how to fix it, but because we have not yet fixed it at the speed life demands.
Still, there are mothers who return again and again, even after disappointment, even after delay. One mother once asked a question that stays long after it is heard: “I came. Why was it not enough?” And in that question lives the entire gap between intention and impact, between presence and protection. Because a child does not get a second chance at being born HIV-free. There is no rehearsal for birth, no second attempt for systems that arrive too late.
Women living with HIV carry knowledge shaped by lived reality—knowledge of survival, adherence, stigma, and resilience. Yet too often their voices are acknowledged but not resourced. Support groups are mentioned but underfunded, consulted but not strengthened. And yet there is truth in community: “Umoja ni nguvu”—unity is strength. Without investment in that unity, it remains only a phrase rather than a system of protection.
If we are serious—truly serious—then the next pregnant or breastfeeding mother must encounter a system that is ready before she arrives: ART available without delay, care that is continuous rather than fragmented, respect that replaces judgment, and peer support that is funded rather than symbolic. Because delay is never neutral; it always chooses its outcome, and in this epidemic, that outcome is measured in children.
There is a proverb: “Tomorrow is pregnant; no one knows what it will give birth to.” But in public health, tomorrow is shaped by today’s decisions. We already know what works. We already know what must change. The question is no longer understanding—it is action. Because 3,396 children are not just a number. They are a story still being written. And Kenya must decide whether that story continues as avoidable loss, or becomes the moment we finally chose to end it.
- Health
- Global